.webp)
He had done everything right.
The psychiatric evaluation was thorough.
The diagnosis aligned with DSM-5-TR criteria.
Medication was initiated according to clinical practice guidelines.
Psychotherapy referral was placed.
Follow-up intervals were guideline-consistent.
Yet six months later, the patient had been hospitalized twice.
Three medication trials had been attempted.
Two augmentation strategies were added.
Sleep worsened. Function declined. Costs escalated.
The uncomfortable question was not whether clinical practice guidelines were followed.
It was whether following multiple clinical practice guidelines simultaneously had quietly made care more complicated than therapeutic.
This tension defines modern psychiatry.
.webp)
Clinical Practice Guidelines and the Rise of Algorithmic Psychiatry
Over the past two decades, clinical practice guidelines have multiplied across psychiatric subspecialties. Organizations such as the APA, CANMAT, NICE, VA/DoD, the Maudsley Prescribing Guidelines, and ASAM have developed increasingly detailed treatment algorithms covering nearly every diagnostic and treatment scenario.
This expansion has brought measurable benefits. Studies suggest that guideline-concordant care improves remission rates in major depressive disorder by up to 20-30% compared to non-standardized treatment pathways, while reducing inappropriate prescribing patterns. Guideline use has also been associated with improved medication safety monitoring and earlier identification of treatment-resistant illness.
However, this proliferation has introduced a new challenge.
Clinicians are no longer navigating a single framework. They are navigating multiple overlapping clinical practice guidelines, each with its own evidence hierarchy, sequencing logic, and safety emphasis.
The result is not simply standardization.
It is algorithm density.
Clinical Practice Guidelines and the Cognitive Load Crisis
Psychiatry is already a cognitively demanding discipline. A typical psychiatric evaluation requires simultaneous integration of diagnostic reasoning, risk assessment, pharmacology, psychosocial formulation, and longitudinal trajectory planning.
The addition of layered clinical practice guidelines has significantly increased this cognitive burden.
Research on clinician burnout consistently shows that documentation demands and decision complexity are major contributors to emotional exhaustion, with psychiatry reporting burnout rates exceeding 40-50% in some workforce surveys. Guideline adherence requirements—often tied to quality metrics and medico-legal defensibility, can amplify this burden by expanding documentation expectations and decision justification requirements.
In practice, clinicians may find themselves spending more time validating decisions against clinical practice guidelines than synthesizing individualized patient formulations.
The paradox is stark.
Guidelines intended to improve clarity may sometimes increase decision friction.
.webp)
Clinical Practice Guidelines and the Cost Escalation Debate
The economic implications of guideline expansion remain controversial. Evidence-based treatment sequencing can reduce relapse-related hospitalization costs. For example, guideline-supported early clozapine initiation in treatment-resistant schizophrenia has been shown to reduce long-term healthcare expenditures by decreasing rehospitalization rates.
Yet guideline adherence can also drive short-term cost escalation through:
Increased laboratory monitoring requirements
Expanded polypharmacy during augmentation phases
Longer consultation times
More frequent follow-up visits
Structured psychotherapy integration mandates
In the United States, mental health expenditures have risen significantly over the past decade, with prescription psychotropic spending alone reaching tens of billions annually. Some health economists argue that strict algorithmic adherence without clinical prioritization may unintentionally promote treatment layering rather than treatment optimization.
The debate is not about whether clinical practice guidelines improve care.
It is about whether they sometimes increase system strain before long-term benefits emerge.
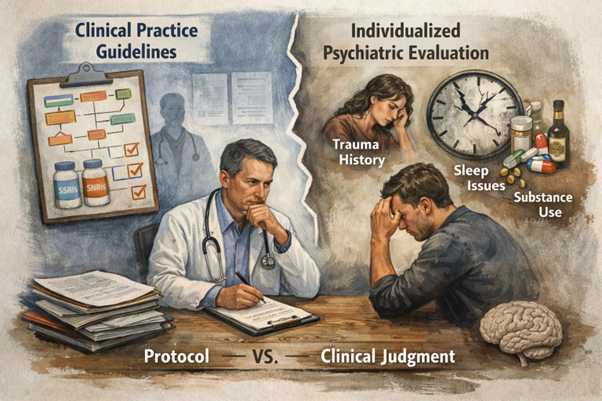
Clinical Practice Guidelines vs Individualized Psychiatric Evaluation
A central tension in psychiatry lies between population-level evidence and individual patient variability.
Clinical trials informing major clinical practice guidelines typically exclude complex comorbidities, severe psychosocial instability, and real-world adherence variability. Yet these are precisely the conditions encountered during routine psychiatric evaluation.
Consider a patient with generalized anxiety disorder who has failed two SSRI trials due to sexual dysfunction and sedation. CANMAT and APA clinical practice guidelines may recommend switching to an SNRI or considering augmentation strategies. However, comorbid trauma history, circadian rhythm disruption, and substance use patterns may alter pharmacodynamic response.
Rigid algorithm application without contextual synthesis risks transforming psychiatry into checklist medicine rather than interpretive medicine.
This concern has been echoed in professional commentary emphasizing that clinical practice guidelines are tools, not replacements for clinical judgment.
Clinical Practice Guidelines and Polypharmacy Momentum
Another unintended consequence of multi-layered guideline pathways is the gradual normalization of complex medication regimens.
Treatment algorithms for major depressive disorder, bipolar disorder, and schizophrenia increasingly include structured augmentation phases. While evidence supports certain combinations, real-world implementation can result in polypharmacy creep, where medications are added faster than they are deprescribed.
Data suggest that up to 30-40% of patients with chronic psychiatric illness receive two or more psychotropic agents concurrently, raising concerns about metabolic burden, drug interactions, and adherence erosion.
Clinical practice guidelines rarely intend to promote indefinite combination therapy. Yet the pressure to demonstrate treatment progression can lead to therapeutic stacking rather than therapeutic clarity.
The risk is subtle.
Guideline fidelity may sometimes outpace outcome evaluation.
.webp)
Clinical Practice Guidelines and Diagnostic Drift
Guideline frameworks rely heavily on accurate diagnostic classification. The DSM-5-TR provides operationalized criteria, but psychiatric syndromes evolve over time.
Patients initially diagnosed with recurrent major depression may later exhibit bipolar spectrum features. Anxiety disorders may mask neurodevelopmental conditions. Substance-induced symptoms may mimic primary psychiatric illness.
When clinical practice guidelines are applied to evolving diagnoses, treatment pathways may inadvertently reinforce incorrect formulations. Sequential medication trials based on an incomplete diagnostic model can increase both cost and patient morbidity.
This phenomenon underscores a critical principle:
Guidelines optimize treatment after diagnosis is clarified.
They cannot compensate for diagnostic uncertainty.
Clinical Practice Guidelines and the Defensive Psychiatry Question
In increasingly regulated healthcare environments, guideline adherence has become intertwined with medico-legal protection.
Documentation referencing APA, CANMAT, or ASAM clinical practice guidelines may strengthen justification for prescribing decisions. Quality assurance systems frequently evaluate whether treatment aligns with established protocols.
While this trend improves accountability, it may also contribute to defensive psychiatry, where treatment sequencing is influenced as much by compliance considerations as by clinical intuition.
Clinicians may feel compelled to follow algorithmic steps even when experiential knowledge suggests alternative strategies.
The question is not whether guidelines protect clinicians.
It is whether they sometimes constrain therapeutic flexibility.
Clinical Practice Guidelines Across Special Populations
Guideline complexity increases further when applied to geriatric, pediatric, and substance-use populations.
Age-related pharmacokinetic changes necessitate slower titration and stricter monitoring. Developmental considerations influence medication approvals in youth. ASAM clinical practice guidelines for withdrawal management require dynamic dosing adjustments based on evolving physiological states.
Each additional framework enhances safety but also multiplies decision variables.
Psychiatry becomes not a single algorithmic pathway but a multidimensional protocol landscape.
Navigating this landscape requires both knowledge depth and cognitive bandwidth.
.webp)
Clinical Practice Guidelines: Why They Still Matter
Despite these tensions, the value of clinical practice guidelines remains profound.
Guidelines reduce unwarranted treatment variability.
They improve early recognition of treatment resistance.
They promote evidence-based psychotherapy integration.
They standardize safety monitoring for high-risk medications.
They support trainee education and interdisciplinary coordination.
In conditions such as schizophrenia, bipolar disorder, PTSD, and substance use disorders, guideline-informed care is associated with improved functional outcomes and reduced relapse rates.
The challenge is not whether to use clinical practice guidelines.
The challenge is how to use them intelligently.
Clinical Practice Guidelines and the Future of Psychiatric Decision Support
As guideline complexity grows, clinicians increasingly require structured systems to synthesize recommendations across organizations, diagnoses, and phases of care.
This is where emerging models such as the psychiatric clinical co-pilot concept are gaining attention.
Platforms like On-Demand Psychiatry are designed to integrate APA, CANMAT, NICE, VA/DoD, ASAM, and DSM-5-TR logic into real-time decision support workflows. Rather than replacing clinical reasoning, these tools aim to reduce cognitive overload by:
Aligning treatment sequencing with guideline evidence tiers
Flagging safety monitoring requirements
Supporting phase-specific treatment planning
Generating structured documentation rationales
Helping clinicians prioritize among competing guideline pathways
The goal is not automation.
It is clinical clarity.
Conclusion: Safety Framework or Cognitive Overload?
Psychiatry stands at a crossroads.
We have more clinical practice guidelines than at any point in history.
We have stronger evidence bases.
Better medications.
More psychotherapy models.
Greater regulatory oversight.
Yet clinicians also face rising burnout.
Patients face increasing treatment complexity.
Healthcare systems face escalating costs.
Guidelines have made psychiatry safer.
But safety without synthesis can become burden.
The future will not belong to those who reject guidelines.
Nor to those who follow them blindly.
It will belong to those who can integrate evidence with judgment, algorithms with intuition, and structure with adaptability.
Because in the end, psychiatric care is not delivered by guidelines.
It is delivered by clinicians navigating them.

FAQ: Clinical Practice Guidelines in Psychiatry
Are clinical practice guidelines mandatory in psychiatric care?
They are not legally mandatory in most settings but strongly influence standards of care, quality metrics, and medico-legal defensibility.
Do clinical practice guidelines improve patient outcomes?
Yes. Guideline-concordant treatment has been associated with improved remission rates, better safety monitoring, and reduced relapse in several psychiatric disorders.
Can strict adherence to clinical practice guidelines increase treatment complexity?
Potentially. Multiple overlapping guidelines may increase cognitive load, documentation demands, and polypharmacy risk if not applied with individualized clinical reasoning.
How should clinicians balance guidelines with patient-specific factors?
Guidelines should inform but not replace comprehensive psychiatric evaluation, longitudinal assessment, and shared decision-making.
What role can decision-support tools play in guideline navigation?
Psychiatric clinical co-pilot systems can help synthesize recommendations across organizations, improving efficiency while preserving clinician autonomy.
This article is intended for licensed healthcare professionals. It does not provide medical advice, diagnose conditions, or substitute for clinical judgment. All clinical decisions must be made by a qualified clinician familiar with the individual patient. For emergencies, call 911. For mental health crisis support in the US, call or text 988.
.webp)