The Uncomfortable Question Psychiatry Must Face
What if the most important intervention in psychiatry is quietly deteriorating?
Not medication.
Not psychotherapy.
Not even access.
The psychiatric evaluation.
In modern clinical practice, the psychiatric evaluation, once the intellectual backbone of diagnosis and treatment, is increasingly compressed into rushed templates, fragmented documentation, and symptom checklists masquerading as clinical reasoning. Mental health assessment has never been more necessary, yet in many settings it has never been more vulnerable.
This is controversial to say.
But it is becoming harder to ignore.
A psychiatric evaluation today often determines whether a patient receives the correct diagnosis, the right medication, or a trajectory toward recovery or toward years of mislabeling, polypharmacy, and preventable risk. When psychiatric evaluation quality declines, downstream consequences multiply quietly.
According to the World Health Organization, depression alone affects over 280 million people globally, making diagnostic precision not a theoretical ideal but a public health necessity. Meanwhile, the National Institute of Mental Health notes that nearly one in five U.S. adults experiences a mental illness each year, placing enormous pressure on clinicians to conduct accurate psychiatric evaluation and comprehensive mental health assessment in time-limited settings.
The uncomfortable reality is this:
Modern psychiatry is not suffering from a lack of knowledge.
It is increasingly struggling with the execution of psychiatric evaluation under pressure.
And that execution gap is shaping outcomes more than most clinicians realize.
Psychiatric Evaluation vs Symptom Listing: A Growing Clinical Divide
A true psychiatric evaluation is not a symptom inventory.
It is a disciplined clinical synthesis, an integration of history, course of illness, functional impact, risk assessment, medical contributors, psychosocial context, and treatment response patterns. Mental health assessment that fails to synthesize these dimensions risks reducing complex human illness into fragmented data points.
Psychiatric evaluation requires pattern recognition.
Yet modern documentation structures often reward completeness over coherence. Clinicians may record dozens of symptoms while missing the narrative arc that defines diagnosis. This phenomenon sometimes referred to informally as “checklist psychiatry” reflects a broader systems tension: efficiency metrics versus clinical reasoning depth.
The American Psychiatric Association has repeatedly emphasized the importance of comprehensive assessment in diagnostic formulation. As DSM-5-TR development leaders noted, psychiatric diagnosis is “not merely descriptive but interpretive, requiring clinical judgment across time and context.”
When psychiatric evaluation becomes superficial, mental health assessment becomes reactive rather than anticipatory. Treatment plans may address isolated complaints instead of underlying syndromes.
And the cost of that gap is rarely immediate but often profound.
Real-World Scenario: When Psychiatric Evaluation Is Rushed
Consider a patient presenting with persistent depressive symptoms, insomnia, and functional decline. A rapid psychiatric evaluation labels the condition as major depressive disorder, leading to sequential antidepressant trials.
Months later, agitation, impulsivity, and mood instability emerge. Collateral history reveals episodic hypomanic symptoms that were never explored during initial mental health assessment.
The diagnosis shifts to bipolar spectrum illness.
What followed was not just a diagnostic delay.
It was a cascade:
Medication-induced destabilization
Occupational impairment
Relationship breakdown
Increased suicide risk
Premature diagnostic closure during psychiatric evaluation is not uncommon. Research suggests that bipolar disorder is frequently misdiagnosed for years, contributing to treatment resistance and functional decline.
The controversy is not that clinicians lack skill.
It is that psychiatric evaluation is increasingly performed under structural constraints that reward speed over synthesis.
The Documentation Paradox in Psychiatric Evaluation
Modern psychiatric evaluation must serve multiple purposes simultaneously:
Clinical communication
Legal defensibility
Billing compliance
Continuity of care
Risk documentation
Mental health assessment notes have become longer, yet sometimes less clear.
Over-documentation can obscure reasoning.
Under-documentation can undermine safety.
A well-structured psychiatric evaluation should answer three critical questions:
What is happening clinically?
Why is it happening now?
What is the safest and most logical next step?
Yet many clinicians report that cognitive bandwidth during psychiatric evaluation is consumed by documentation mechanics rather than diagnostic synthesis.
This tension contributes to variability in mental health assessment quality across settings. Similar patients may receive different diagnoses or treatment pathways depending on clinician workload, institutional protocols, or time constraints.
The debate is not about whether structure is needed.
It is about whether structure is replacing thinking.
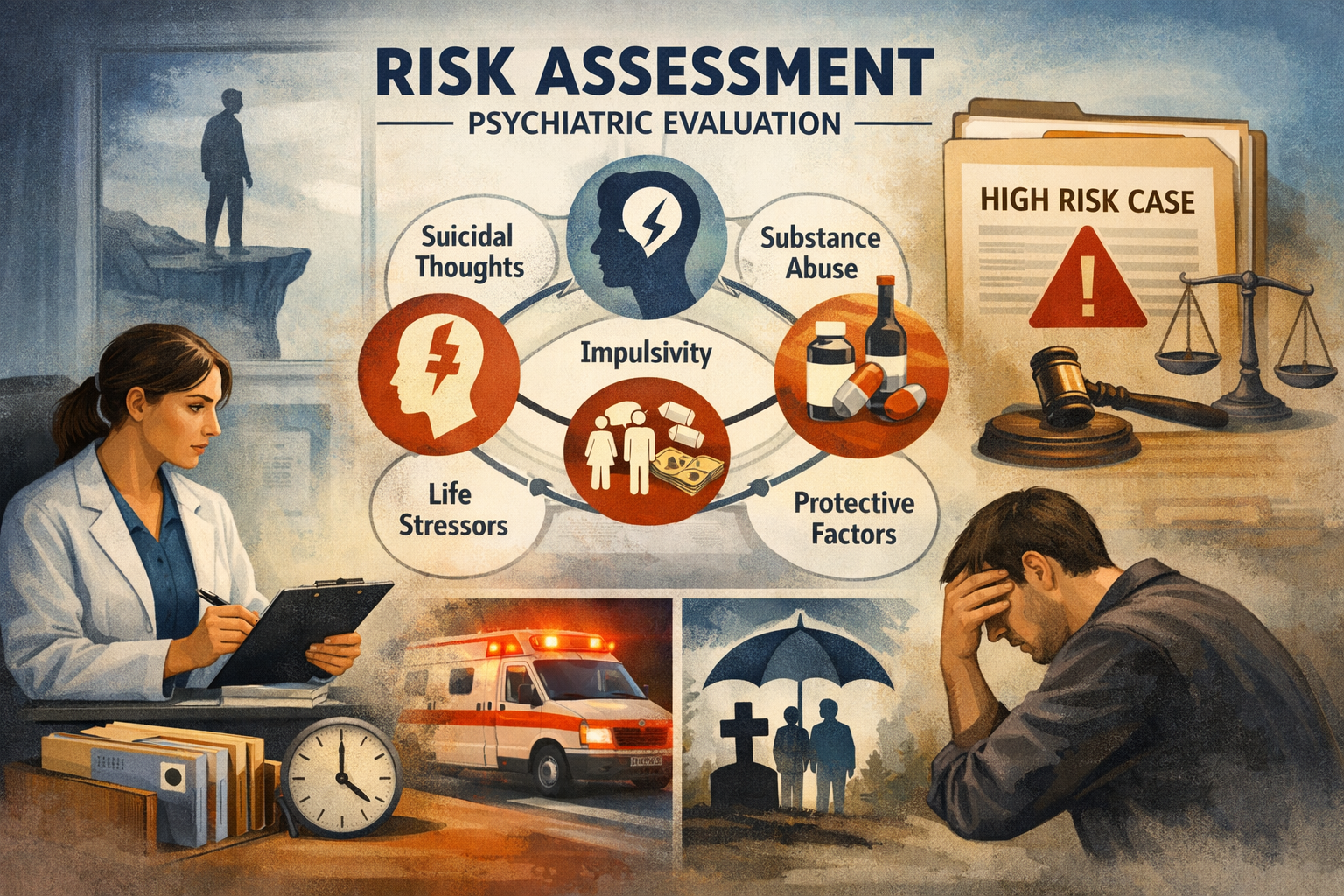
Risk Assessment: The Ethical Core of Psychiatric Evaluation
No component of psychiatric evaluation carries greater weight than risk assessment.
Suicide remains a leading cause of death worldwide. WHO estimates that more than 700,000 people die by suicide each year, underscoring the life-saving potential of accurate mental health assessment.
Yet risk evaluation is not a checkbox exercise.
It requires contextual interpretation:
Trajectory of suicidal ideation
Impulsivity patterns
Substance use influence
Psychosocial stressors
Protective factors
Incomplete psychiatric evaluation in high-risk scenarios can have devastating consequences. Moreover, risk documentation plays a central role in medicolegal review after adverse events.
This reality intensifies the pressure clinicians face, a pressure that further compresses time available for reflective diagnostic reasoning.
Polypharmacy and the Psychiatric Evaluation Crisis
Another controversial dimension of superficial psychiatric evaluation is the emergence of medication layering without clear diagnostic synthesis.
Patients may accumulate multiple psychotropics across fragmented mental health assessments conducted in different settings. Each prescribing decision may appear rational in isolation but incoherent in aggregate.
The result:
Unclear therapeutic targets
Compounded side-effect burden
Diagnostic confusion
Reduced adherence
i=Increased healthcare utilization
As pioneering psychopharmacologist Stephen Stahl has observed, “Prescribing without a clear target symptom cluster is prescribing in the dark.”
Psychiatric evaluation is the mechanism that turns prescribing into precision.
When evaluation quality declines, medication strategy becomes reactive rather than intentional.
Cognitive Overload: The Hidden Driver of Superficial Mental Health Assessment
The psychiatric evaluation crisis is not primarily a knowledge crisis.
It is a cognitive load crisis.
Clinicians must simultaneously track:
Evolving symptom patterns
Prior treatment response
Medical comorbidities
Drug interactions
Risk trajectories
Documentation requirements
Time pressure
Under such conditions, even highly skilled psychiatrists may default to heuristic shortcuts.
This does not reflect incompetence.
It reflects system design.
Harvard physician-researcher Atul Gawande famously noted, “The volume and complexity of what we know has exceeded our individual ability to deliver its benefits correctly.”
Psychiatric evaluation is increasingly subject to this cognitive threshold.
The controversy intensifies here:
Is modern psychiatry unintentionally incentivizing superficial mental health assessment?
A New Approach: Structured Support Without Replacing Judgment
This growing tension has led some clinicians to explore structured reasoning supports, including psychiatry-specific systems often described as psychiatric clinical co-pilots.
Platforms such as On-Demand Psychiatry aim to support psychiatric evaluation by helping clinicians organize diagnostic reasoning, synthesize historical data, structure risk assessment, and generate defensible documentation.
Importantly, such systems do not replace clinical judgment.
They aim to reduce cognitive friction during complex mental health assessment.
In practice, a psychiatric clinical co-pilot may assist clinicians in:
Maintaining diagnostic differentials
Aligning medication decisions with formulation
Structuring risk documentation
Integrating prior records into current psychiatric evaluation
Preserving narrative clarity in time-pressured encounters
The clinician remains fully responsible for diagnosis and treatment decisions.
The debate is not about automation versus expertise.
It is about execution support versus execution erosion.
The Future of Psychiatric Evaluation: Precision Over Volume
The resolution to the psychiatric evaluation crisis does not lie in performing more assessments.
It lies in performing better psychiatric evaluation.
Future mental health assessment models will likely emphasize:
Longitudinal pattern recognition
Structured clinical reasoning frameworks
Integrated documentation
Risk-informed decision pathways
Clinician sustainability
Precision psychiatry is not only about biomarkers or genomics.
It is about disciplined evaluation methodology.
When psychiatric evaluation becomes intentional, treatment becomes coherent.
When mental health assessment is synthesized, outcomes become safer.
And when clinicians are supported rather than overwhelmed, the therapeutic alliance strengthens.
Closing Reflection: Controversy Resolved
The controversy is real.
Modern psychiatric evaluation is under pressure.
Mental health assessment variability is increasing.
Diagnostic execution gaps are shaping outcomes.
Yet this crisis also represents an opportunity.
Psychiatry can evolve toward a model where structured reasoning, thoughtful technology support, and clinician judgment coexist. Psychiatric clinical co-pilots like On-Demand Psychiatry illustrate one possible direction, not as shortcuts, but as tools designed by clinicians to preserve depth in an era of speed.
At its core, psychiatric evaluation remains both science and art.
It demands listening, interpretation, and disciplined synthesis.
If the field protects this process, rather than compressing it, patients will benefit through safer care, clearer treatment pathways, and more reliable recovery trajectories.
The psychiatric evaluation crisis is not the end of thoughtful psychiatry.
It may be the catalyst that strengthens it.
FAQs: Psychiatric Evaluation and Mental Health Assessment
Why is psychiatric evaluation considered the foundation of treatment?
Psychiatric evaluation integrates symptom patterns, history, risk, and functioning into a diagnostic formulation that guides safe and effective treatment planning.
How is psychiatric evaluation different from a symptom checklist?
A checklist records symptoms. A psychiatric evaluation interprets them within context, course, and risk to generate clinical decisions.
What are common errors in mental health assessment?
Premature diagnosis, incomplete risk assessment, medication decisions without synthesis, and unclear documentation are frequent pitfalls.
Can technology improve psychiatric evaluation?
When used thoughtfully, structured tools or psychiatric clinical co-pilots can help clinicians organize reasoning and documentation without replacing judgment.
What defines a high-quality psychiatric evaluation today?
Clarity of formulation, defensible risk assessment, coherent treatment planning, and integration of longitudinal clinical data.
This article is intended for licensed healthcare professionals. It does not provide medical advice, diagnose conditions, or substitute for clinical judgment. All clinical decisions must be made by a qualified clinician familiar with the individual patient. For emergencies, call 911. For mental health crisis support in the US, call or text 988.
.webp)